 24x7 Helpline 080 4019 4444
24x7 Helpline 080 4019 4444Labial Hernia with Ileal Gangrene
Case Studies

A RARE CASE REPORT OF STRANGULATED RIGHT LARGE INGUINO- LABIAL HERNIA WITH GANGRENE OF ILEUM IN SEPSIS.
A rare case report of strangulated right large inguino- labial hernia with gangrene of ileum in sepsis
Authors- Dr Anand Kumar J Team - Dr .Narayan Prasad and Dr Kavya T
Department of General & Laparoscopic Surgery, SUGUNA HOSPITAL.
Discussion and case report
The inguinal canal is traversed by the spermatic cord in men and the round ligament of uterus in women. The round ligament is attached to the uterine cornu near the origin of fallopian tube at one end and to the ipsilateral labia majora at the other. The round ligament accompanies a pouch of parietal peritoneum in the inguinal canal, which is known as ‘canal of nuck’. It is analogous to the processus vaginalis in males. Incomplete obliteration of the peritoneal pouch causes indirect inguinal hernia or hydrocele of the canal of nuck; a very rare condition in women. Long-standing hernia prone for obstruction and strangulation. Hence early detection, aggressive resuscitation, antibiotics and surgical management is treatment. As these types of cases are rarely seen in surgical practice we present this rare case .
- A 67yr old, obese female patient presented to suguna hospital casualty on 20/4/2024 at 10pm, with severe pain abdomen, vomiting, constipation since 2 days, aggravated since 1 day.
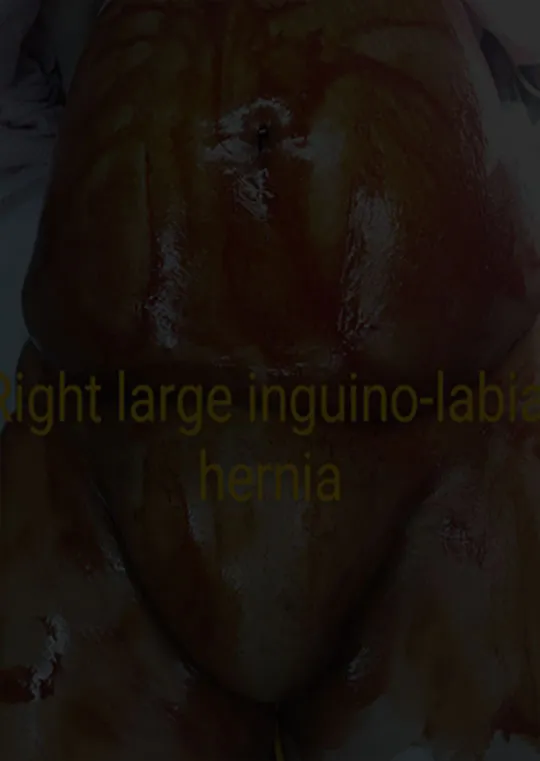
- On examination, patient had tachycardia, tachypnoea with sepsis features and dehydration and features suggestive of peritonitis per abdomen, with large right obstructed, inguino labial hernia with no cough impulse , tense and tender to palpate. Absent bowel sounds.
- Patient was resuscitated immediately in the casualty with IV fluids, IV antibiotics, analgesics.
- Ct scan done outside showed features of ? strangulated right inguino-labial hernia with ? Ischemic changes in bowel in the hernial sac.
- Patient was immediately planned for emergency exploratory Laparotomy, 20/4/2024 midnight, in suguna hospital with out any delay after all pre op work up.
- Surgery- Emergency exploratory Laparotomy, resection anastomosis of gangrene ileum, right inguino labial herniorrhaphy.

Introperatively,
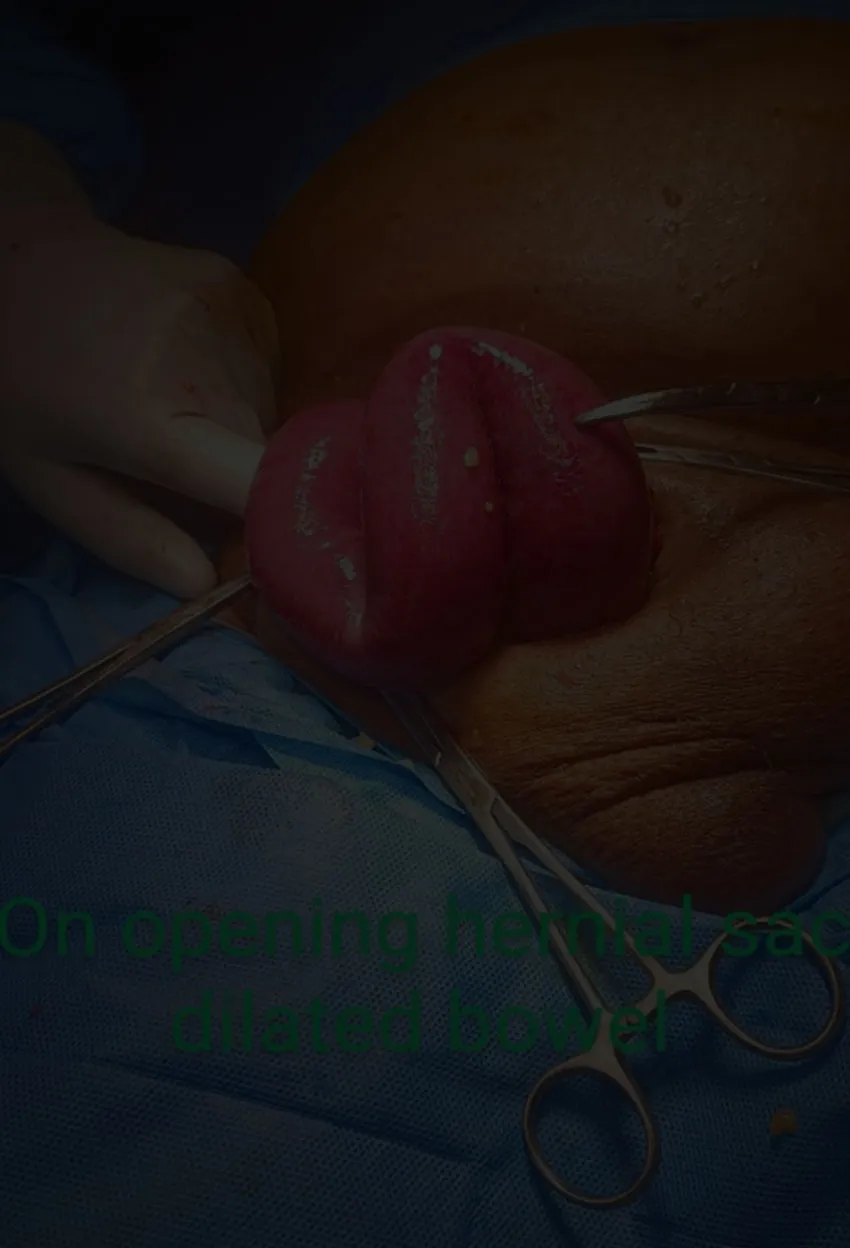
Inguinal incision was taken large tense hernial sac noted, sac was incised noted with 200 ml transudate fluid with dilated small bowel , part of it showed pre ischemic changes. One Loop of small bowel was strangulated in the defect with Frank gangrene, attempt was made to release open the defect, not possible to retrieve the gangrene bowel, hence abdominal Laparotomy incision taken, gangrene bowel released from defect. Rest of dilated bowel loop released from the inguinal defect into the abdomen. At 15 cm from Ileo cecal junction, 15 cm of ileum was found gangrenous . Resection anastomosis of gangrene bowel done. Abdomen wound closed in layers. Inguinal hernial defect anatomical repair done .
Post procedure, patient shifted to ICU for elective extubation. Patient is doing fine, post op day 1 ambulated out of bed, sepsis features subsided and hemodynamically stable and doing well.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}